In the modern surgical suite, the hazards of surgical smoke—plumes generated by lasers, electrosurgical units (ESU), cauteries and ultrasonic devices are well-documented. Containing over 147 hazardous chemicals and viable biological particulates, including live viruses, this “byproduct” is a significant occupational health risk for dermatologists, nurses, and technicians.
To mitigate this risk, smoke evacuators are essential. However, not all filtration systems are created equal or designed for surgical or clinical use. While HEPA (High-Efficiency Particulate Air) filters have long been the industry standard for room air filtration, ULPA (Ultra-Low Penetration Air) filters represent the ultimate in surgical smoke protection.
At Acuderm, our Evac systems utilize ULPA technology combined with carbon for gas and odor removal. Here is a technical breakdown of why ULPA filtration—specifically those rated at 99.99997% efficiency—is the superior choice for your practice.
The Fundamental Difference: HEPA vs. ULPA
The distinction between HEPA and ULPA lies in the “tightness” of the filter media and the size of the particles they are validated to capture.
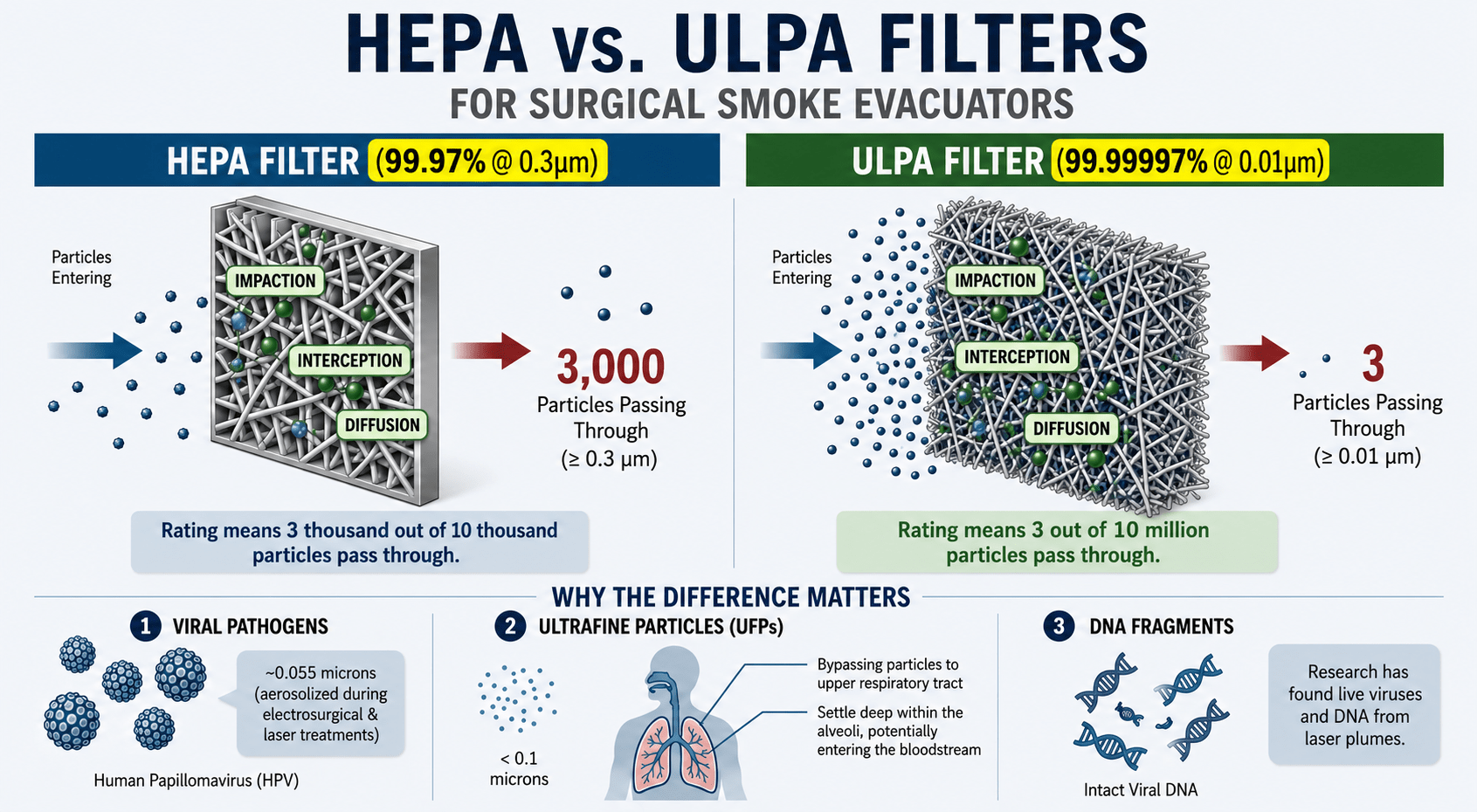
- HEPA Filters: Typically rated to capture 99.97% of particles at 0.3 microns.
- ULPA Filters: Rated to capture 99.99997% at 0.01 microns and 0.12 microns MPPS (Most Penetrating Particle Size).
Why the 0.01 to 0.12 Micron Range Matters
In dermatology and laser surgery, the “targets” we aim to capture are often much smaller than the 0.3-micron HEPA benchmark.
- Viral Pathogens: The Human Papillomavirus (HPV), frequently aerosolized during the treatment of verrucae or condyloma, measures approximately 0.055 microns. A HEPA filter is not validated to capture particles of this size with the same efficiency as an ULPA filter.
- Ultrafine Particles (UFPs): Laser plumes produce a high concentration of ultrafine particles (less than 0.1 microns). These particles can bypass the upper respiratory tract and settle deep within the alveoli of the lungs, potentially entering the bloodstream.
- DNA Fragments: Research has shown that intact viral DNA and live viruses was recovered from laser plumes. ULPA filters provide the necessary density to ensure these fragments are sequestered within the filter media.
Pathogen Size Comparison Chart
| Pathogen | Particle Size (Microns) | Captured by Acuderm ULPA? |
|---|---|---|
| Hepatitis A | 0.027 – 0.032 | Yes |
| Hepatitis B | 0.042 | Yes |
| Hepatitis C | 0.04 – 0.08 | Yes |
| HPV | 0.05 – 0.055 | Yes |
| SARS-CoV-2 | 0.05 – 0.14 | Yes |
| HIV | 0.12 | Yes |
Quantifying the Efficiency: The Math of Safety
The certified difference between 99.97% (HEPA) and 99.99997% (Acuderm’s ULPA) is a massive leap in clinical safety:
- HEPA (99.97%): Allows 3,000 out of every 10,000,000 particles at 0.3 microns to pass through.
- Acuderm’s ULPA (99.99997%): Allows only 3 out of every 10,000,000 particles at 0.01 micron to pass through.
In a high-volume dermatology clinic, this 1,000-fold increase in protection significantly reduces cumulative exposure for the surgical team.
Why do Gas and Odor Matter?
Gases and odors from surgical smoke are not only toxic and mutagenic to breathe; they irritate the eyes, nose, throat and lungs.
Clinical Indicator: The presence of odor is an indicator that your surgical smoke evacuator is not working as indicated.
HEPA filters have no effect on gases and odors. Acu-Evac’s Main Filter combines the highest level of filtration available with its ULPA filter and a specially designed carbon filter to remove harmful gases and odors.
Implications for the Clinical and Surgical Team
For the physician, nurse, and laser technician, the use of the Acu-Evac means:
- Protection Starts with Capture: The TX Nozzle was issued 3 patents because of its superior capture of surgical smoke at the source.
- Superior Odor Control: ULPA filters are paired with advanced charcoal filtration to remove harmful gases such as Volatile Organic Compounds (VOCs), benzene, and odors.
- Infection & Cross-Contamination Control: By capturing smoke with blood droplets and particulates down to the 0.01-micron level, the risk of viable biological material remaining in the room air is virtually eliminated.
Conclusion
While HEPA is suitable for general room air filtration, the specialized environment of a medical or surgical suite where electrosurgical units (ESU), cautery, laser or ultrasonic devices are used demands the precision of ULPA. By choosing the only surgical smoke evacuator to be awarded a US Patent & in 15 countries and a capture nozzle to be awarded 3 US Patents, you are choosing the highest possible standard of respiratory protection.
After all, isn’t your health and well-being worth it?
Upgrade Your Practice: View the Acuderm Evac Series Specifications Here
Sources:
Provided client text and technical specifications from Acuderm.com/evac.
NIOSH (National Institute for Occupational Safety and Health) – Research on Surgical Smoke Hazards.
ANSI/AAMI ST108:2023 – Water for the processing of medical devices (Principles for air quality and filtration).
Journal of the American Academy of Dermatology (JAAD) – Studies on HPV DNA in laser plumes.
Yeh, C. (1997). Surgical Smoke Plume: Principles and Function of smoke, aerosol, gases and smoke evacuation. Surgical Services Management (3)4:41.


